Five next-generation TKIs — osimertinib, lorlatinib, alectinib, repotrectinib, and selpercatinib — now occupy the first-line slot across the actionable driver landscape in metastatic NSCLC. The question has shifted from whether to test to which platform, for which mutation, and what to do at progression.
01 · DiagnosticsThe Biomarker Floor
Comprehensive genomic profiling — ideally tissue-based NGS plus reflex liquid biopsy at progression — is no longer optional. The minimal actionable panel covers EGFR, ALK, ROS1, BRAF, MET ex14, RET, NTRK, KRAS G12C, HER2, and increasingly NRG1 fusions. Centres that defer testing for “small samples” routinely miss 8–12% of actionable alterations later confirmed on rebiopsy.
Turn-around-time discipline matters as much as panel breadth: a 14-day SLA from biopsy to multidisciplinary tumour-board review correlates with substantially higher first-line targeted-therapy uptake.
02 · EGFREGFR-Mutant Disease: Combination Pressure on Monotherapy
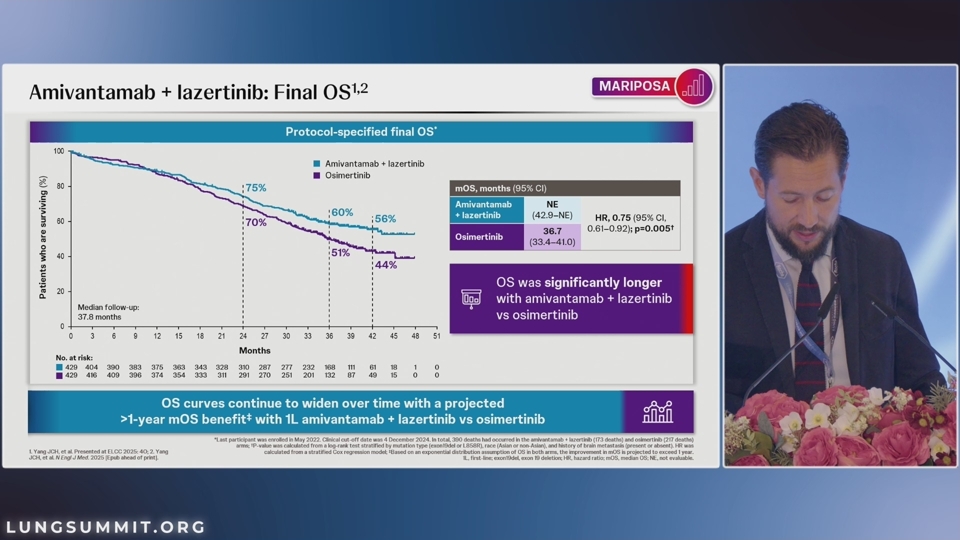
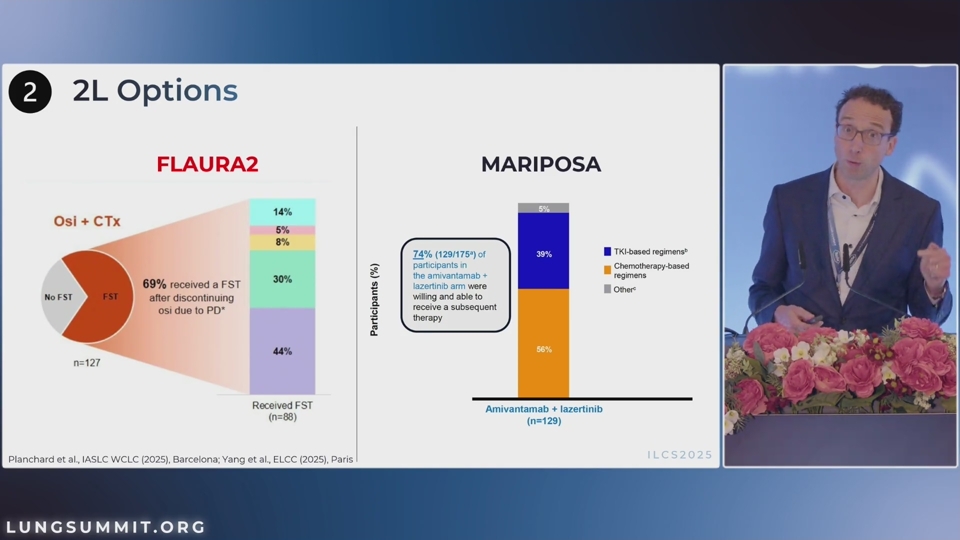
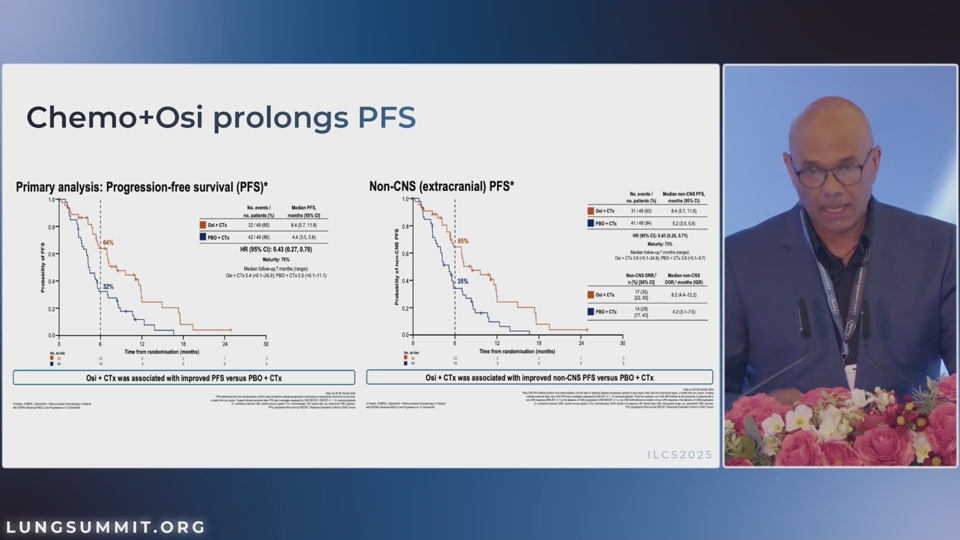
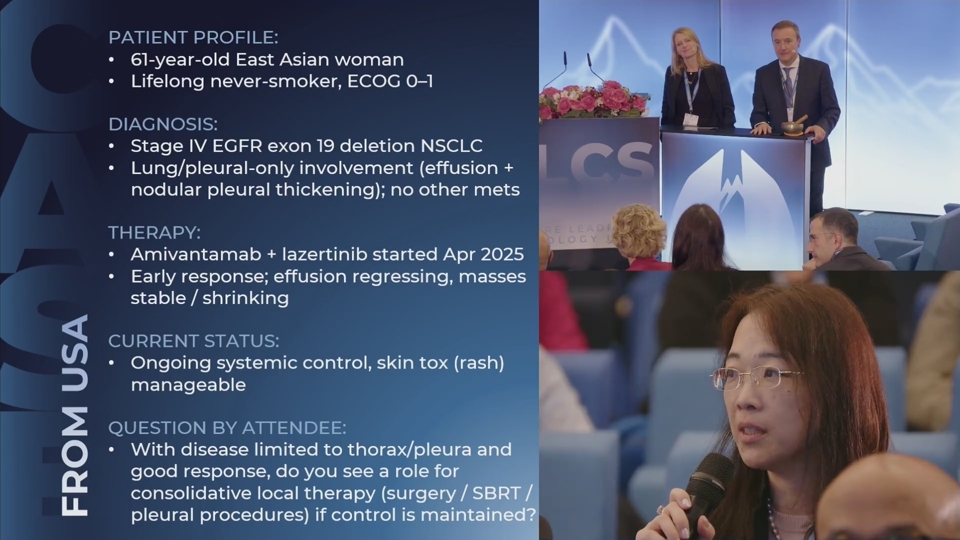
Osimertinib monotherapy remains the most-prescribed first-line option, but two phase-3 readouts in 2024–25 have created legitimate combination alternatives. FLAURA2 (osimertinib + platinum-pemetrexed) and MARIPOSA (amivantamab + lazertinib) each extend PFS over single-agent osimertinib, at the cost of meaningful toxicity escalation.
For a fit patient with brain-only metastatic disease and an exon-19 deletion, osimertinib monotherapy still gives me the best therapeutic index. The combinations earn their place in higher-risk subgroups — bulky thoracic disease, L858R, baseline TP53.
— Solange Peters, MD · ILCS 2025 plenary
02.1CNS Activity as a Decision Driver
Across the EGFR field, intracranial response rates favour osimertinib-containing regimens over chemotherapy backbones. For patients presenting with symptomatic CNS disease, this often outweighs the modest systemic PFS gain seen with combinations.
03 · ALK + ROS1ALK and ROS1: A New Standard Each
Lorlatinib displaced alectinib as the dominant first-line ALK choice after the 5-year CROWN update, with median PFS still not reached. For ROS1, repotrectinib’s CNS coverage and TKI-naïve activity in solvent-front mutations have moved it into the first-line slot ahead of crizotinib and entrectinib.
Key takeaways
What to remember
- Comprehensive NGS at diagnosis is the gating step — defer everything else until results land.
- Osimertinib monotherapy remains the default first-line in classical EGFR; combinations earn their place in high-risk subgroups.
- Lorlatinib is now the de facto first-line ALK option; repotrectinib leads in ROS1.
- Plan the second-line move at the point of first-line prescription — resistance landscape varies dramatically by mutation class.
ReferencesSelected Reading
- Solomon BJ et al. Lorlatinib versus crizotinib in advanced ALK-positive NSCLC: 5-year analysis of CROWN. J Clin Oncol. 2025.
- Planchard D et al. FLAURA2 final OS analysis. Lancet Oncol. 2025.
- Cho BC et al. MARIPOSA: amivantamab + lazertinib vs osimertinib in first-line EGFR-mutant NSCLC. N Engl J Med. 2024.
- Drilon A et al. Repotrectinib in ROS1-positive NSCLC: TRIDENT-1 update. N Engl J Med. 2024.