Three randomised phase-3 trials have now shifted resectable, stage II–IIIA NSCLC into a perioperative chemo-immunotherapy era. This practice update distils the evidence, the open questions, and a working algorithm for the multidisciplinary clinic.
01 · BackgroundSetting the Stage
For two decades, adjuvant cisplatin-based chemotherapy delivered a modest 5% absolute overall-survival benefit in fully resected stage II–IIIA non-small-cell lung cancer (NSCLC). That ceiling has been broken. With CheckMate 816, KEYNOTE-671, AEGEAN and CheckMate 77T all reporting positive event-free survival, the centre of gravity has moved from adjuvant alone to a perioperative paradigm — neoadjuvant chemo + immune-checkpoint inhibitor (ICI), followed by surgery, followed by adjuvant ICI.
The clinical question is no longer whether to use immunotherapy in resectable disease, but which platform, for which patient, and for how long.
02 · Pivotal dataNeoadjuvant Evidence: CheckMate 816 and Beyond
CheckMate 816 was the first phase-3 trial to demonstrate a pathological complete response (pCR) advantage with neoadjuvant nivolumab + chemotherapy versus chemotherapy alone (24.0% vs 2.2%) and improved event-free survival (HR 0.63). Five-year follow-up presented at ILCS 2025 confirms a sustained overall-survival benefit, with the largest gains concentrated in PD-L1 ≥ 1% and stage IIIA disease.
The CheckMate 816 update at five years is the strongest evidence we have that neoadjuvant ICI changes the natural history of resectable NSCLC — not just its imaging response.
— Alessandra Curioni, MD · ILCS 2025

Figure 1 · ILCS 2025 Faculty Panel
03 · ComparisonPerioperative Platforms
KEYNOTE-671 (pembrolizumab), AEGEAN (durvalumab) and CheckMate 77T (nivolumab) extend the CheckMate 816 design by adding an adjuvant ICI phase. All three have read out positive on the primary EFS endpoint, with hazard ratios clustered between 0.58 and 0.68.
Cross-Trial Caveats
- Distinct PD-L1 cut-points and assay platforms across trials limit head-to-head interpretation.
- Surgery rates were higher in CheckMate 816 than in the perioperative trials — a function of patient selection, not regimen.
- Adjuvant phase completion rates hovered around 60–70%, raising questions about the marginal benefit of the post-operative phase.
- Overall-survival data remain immature for the perioperative trials.
Key Takeaways
What to Take Into Clinic Tomorrow
- Perioperative chemo-ICI is the new standard for resectable stage II–IIIA NSCLC without driver alterations.
- Neoadjuvant-only (CheckMate 816) remains a reasonable option when adjuvant burden is a concern.
- EGFR and ALK alterations should be tested before neoadjuvant therapy — ICI is contraindicated and adjuvant TKI is preferred.
- Multidisciplinary review at diagnosis is non-negotiable.
04 · Patient selectionSelecting Patients
Driver-alteration testing has moved upstream. EGFR, ALK, ROS1 and KRAS-G12C should be assessed on the diagnostic biopsy before any treatment decision — not after surgery. ICI exposure in an EGFR-mutant patient delays effective targeted therapy and risks autoimmune toxicity once a TKI is introduced.
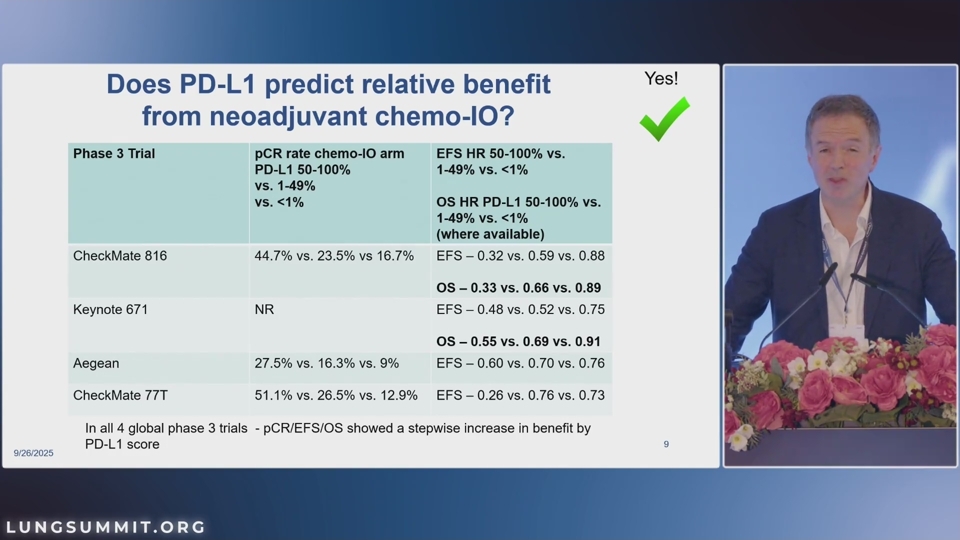
PD-L1, Biomarkers, MRD
PD-L1 expression remains the most actionable predictor of magnitude of benefit. Tumour mutational burden, gene-expression signatures, and circulating-tumour-DNA (ctDNA) dynamics are accumulating evidence as response-adaptive tools, but none yet meet the bar for standalone clinical decision-making outside a trial.
05 · SurgerySurgical Considerations
Resectability is a moving target. The IO era has expanded the indication envelope — borderline-resectable tumours may downstage to a complete resection — but surgeons must navigate a denser, more fibrotic operative field after three cycles of chemo-ICI. Operative timing (typically within 6 weeks of cycle 3) and the choice of lobectomy versus sleeve resection should be re-discussed at multidisciplinary tumour board after restaging.
06 · Open questionsAdjuvant Questions That Remain
The marginal contribution of the adjuvant ICI phase, optimal duration, and whether ctDNA can rationalise de-escalation are the three most active research questions in 2026. Trials including MERMAID-1, MRD-1, and the IFCT-PINnaCLE adaptive platform will inform practice over the next 24 months.
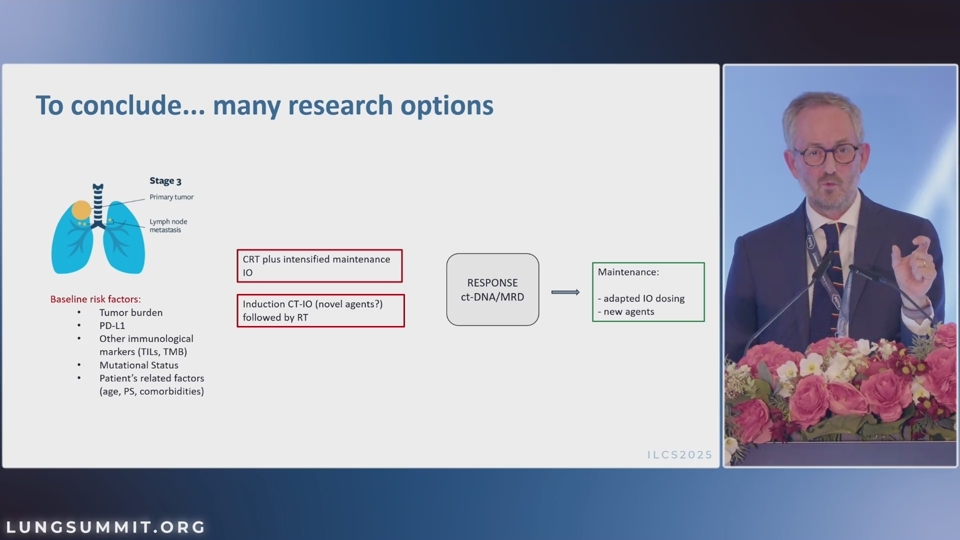
07 · AlgorithmA Practical Algorithm
For a fit patient with stage II–IIIA, driver-negative NSCLC and PD-L1 ≥ 1%, our default is perioperative pembrolizumab or nivolumab + chemotherapy. For patients with high adjuvant-burden risk or limited compliance, CheckMate 816 neoadjuvant-only is a reasonable de-intensified path. Stage I disease remains outside this algorithm pending CheckMate 77T sub-group readouts.
- Biopsy with full molecular panel — EGFR, ALK, ROS1, KRAS, BRAF, MET, RET, NTRK, PD-L1.
- Multidisciplinary review including thoracic surgery, medical oncology, radiation oncology and pathology.
- If driver-negative and PD-L1 ≥ 1%: perioperative chemo-ICI × 3–4 cycles → surgery → adjuvant ICI to one year.
- If driver-positive: targeted-therapy adjuvant strategy; ICI is not indicated.
- Restaging at cycle 3 with PET-CT and brain MRI before surgical scheduling.
This educational article is part of the Lung Summit Reading Room, produced under unrestricted editorial control by the ILCS faculty. CME activity supported by an independent medical-education grant from Bristol Myers Squibb. Authors’ full disclosure statements are linked in each faculty card above.
References
- Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386(21):1973–1985.
- Wakelee H, Liberman M, Kato T, et al. Perioperative pembrolizumab for early-stage non-small-cell lung cancer. N Engl J Med. 2023;389(6):491–503.
- Heymach JV, Harpole D, Mitsudomi T, et al. Perioperative durvalumab for resectable non-small-cell lung cancer. N Engl J Med. 2023;389(18):1672–1684.
- Cascone T, Awad MM, Spicer JD, et al. Perioperative nivolumab in resectable lung cancer (CheckMate 77T). N Engl J Med. 2024;390(18):1672–1684.
- Spicer JD, Cascone T, Wynes MW, et al. Neoadjuvant and adjuvant treatments for early-stage resectable NSCLC: consensus recommendations from the IASLC. J Thorac Oncol. 2024;19(3):385–409.